Dialysis Access (Vascular Access for Hemodialysis)
Overview & Importance
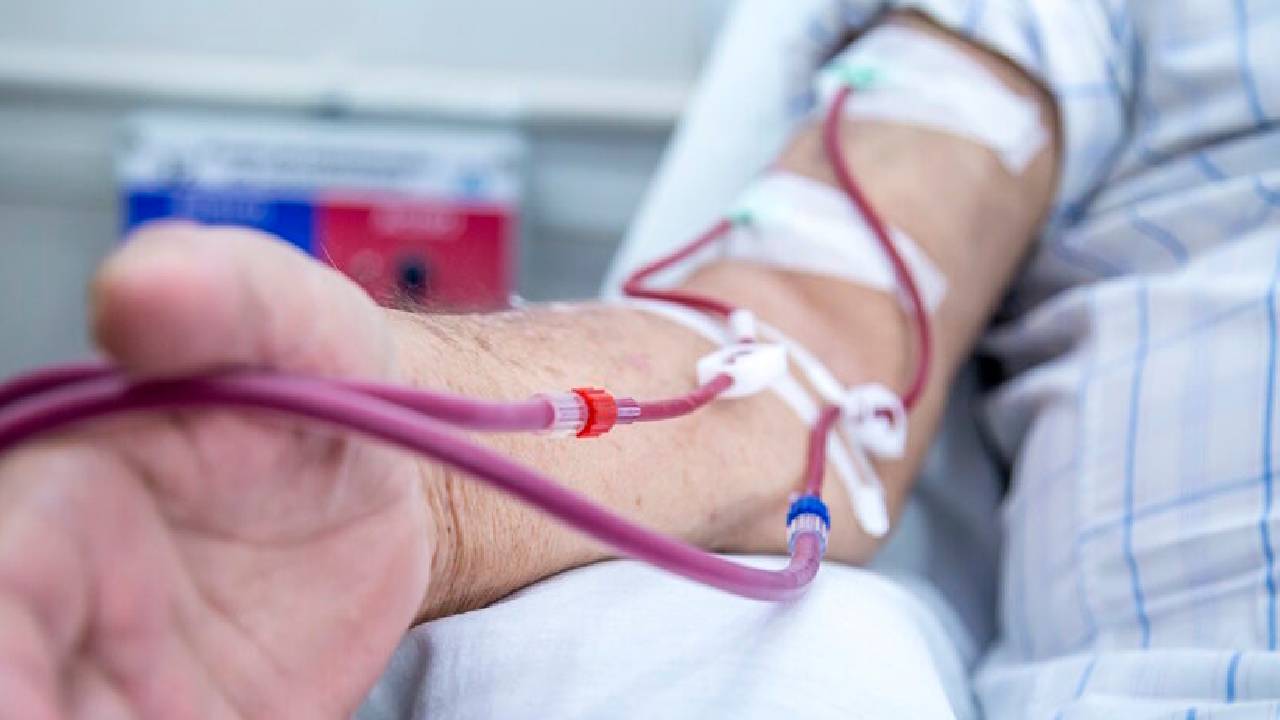
In patients with end-stage renal disease (ESRD) who require hemodialysis, a reliable vascular access is essential because dialysis requires high flows of blood into and out of the body.
The access must allow repeated, high-volume flows (300–500 mL/min or more), be durable, and minimize complications (clotting, infection, limb ischemia).
Because of these demands, creating and maintaining dialysis access is a major component of vascular surgery and interventional practice.
Types of Access & Their Characteristics
The fistula is considered the “gold standard” for long-term vascular access because it generally offers better durability and fewer complications.
Grafts are used when venous anatomy is not adequate for a fistula.
Catheters are often used as temporary access or when no other access is feasible.
Preoperative Evaluation & Planning
Vein mapping / Duplex ultrasound is essential to select suitable veins and assess arterial inflow.
Evaluate for central venous stenosis if prior catheters or devices were used.
Assess cardiac function; large-flow fistulas can impose additional cardiac load in patients with marginal cardiac reserve.
Plan to preserve veins (avoid venipuncture, IV lines) in the prospective access limb.
Surgical / Interventional Techniques & Maturation
After creating the access (fistula or graft), a maturation period is needed: the vein must dilate and remodel to sustain repeated needle punctures.
If maturation is poor or there is flow-limiting stenosis, interventions such as angioplasty, stenting, thrombectomy, or revision surgery are often required.
In some centers, percutaneous AVF creation techniques (endovascular) are being explored.
Common Complications & Their Management
Thrombosis / Access failure
Narrowing (stenosis) or clot formation can impair flow.
These often require angioplasty, thrombectomy, or revision.
Infection
More common in grafts and catheters.
Management may require antibiotics or removal.
Steal Syndrome / Limb Ischemia
Because some arterial blood is “diverted” into the access, distal ischemia (weakness, pain, numbness) may result.
In severe cases, interventions such as distal revascularization with interval ligation (DRIL), banding, revision using distal inflow (RUDI), or partial ligation are done.
Aneurysm / Pseudoaneurysm formation
Repetitive needling can damage vessel walls.
Failure to mature (“non-maturing” access)
Sometimes the fistula does not dilate sufficiently.
Additional interventions or alternate strategies may be needed.
Ischemic Monomelic Neuropathy
Rare but serious complication: acute neuropathy without overt ischemia, affecting multiple nerve fibers in the limb.
High-flow access / Cardiac strain
Excessive shunting may overload the heart in susceptible patients.
Outcomes & Prognosis
Among access types, long-term patency is best with AV fistula, and outcomes are poorer with catheters (higher rates of hospitalization, complications, and mortality) .
Surveillance (checking the thrill, flow measurements, ultrasound) and prompt intervention on stenoses are critical to prolong access life.
About Dr Pranjal Melge Sawant
Dr Pranjal Melge Sawant is well known General and Vascular Surgeon currently associated with Deenanath Mangeshkar Hospital and Research Center. He has 10 years of experience in General Surgery and worked as an expert General Surgeon in different cities of India. He has worked in many reputed hospitals.